Brain Aneurysms
Specialist neurovascular care in Sydney — a guide for patients and referring GPs

Tap or hover any dotted-underlined term for a plain-English definition.
Most brain aneurysms never bleed. If you’ve just been told you have one, take a breath — there is time to make calm, well-informed decisions. The emergency notice below is for people experiencing acute symptoms right now.
- Most brain aneurysms never rupture. Five-year rupture risk under PHASES ranges roughly from under 1% to over 15%, with small (<7 mm) anterior-circulation aneurysms at the low end and large or posterior-circulation aneurysms at the high end.
- Around 2–3% of adults have an unruptured aneurysm — the vast majority will never know (Vlak et al., Lancet Neurology 2011).
- Modern minimally-invasive treatment — coiling, flow diverters, intrasaccular devices — is done through a small puncture in the wrist or groin. No skull opening is needed for most aneurysms.
- CURA’s neurovascular team personally performs the endovascular procedures — you keep the same specialist from diagnosis through follow-up.
- Rupture risk is individualised using the PHASES scorePHASES scoreA validated tool that estimates 5-year aneurysm rupture risk from six factors: Population, Hypertension, Age, aneurysm Size, Earlier subarachnoid haemorrhage, and Site (location). Greving et al., Lancet Neurology 2014. — size is one variable among six.
You’ve just been told you have an aneurysm — what now?
Today
- Breathe. Most unruptured aneurysms never bleed. You have time to make calm, well-informed decisions.
- If you have a sudden “worst-ever” headache, vomiting, neck stiffness, or sudden weakness — call 000.
- Ask your GP for a copy of your scan and the radiology report (most providers email a USB or grant portal access).
This week
- Ask your GP for a referral to a neurovascular neurologist.
- Check your blood pressure. Bring readings to the consultation.
- If you smoke, this is the moment. Smoking accelerates aneurysm growth and roughly doubles rupture risk.
This month
- Book the consultation. Bring: GP referral, imaging USB or CD, full medication list, blood pressure log, Medicare card.
- You’ll leave with a written plan: surveillance vs treatment, imaging cadence, and the expected next review.
Most incidental aneurysms are non-urgent. Acute symptoms are not — if in doubt, ED first.
What a brain aneurysm is
A brain aneurysm — also called a cerebral or intracranial aneurysm — is a balloon-like bulge in a weakened section of artery wall.
Most form at branch points where blood vessels divide. The classic sites are the anterior communicating artery, the posterior communicating artery, the middle cerebral artery (MCA) bifurcation, the paraclinoid internal carotid artery, and the basilar tip — arteries that together form the circle of WillisCircle of WillisThe ring of arteries at the base of the brain that share blood between the brain’s left, right, front and back regions. at the base of the brain.
Three shapes matter:
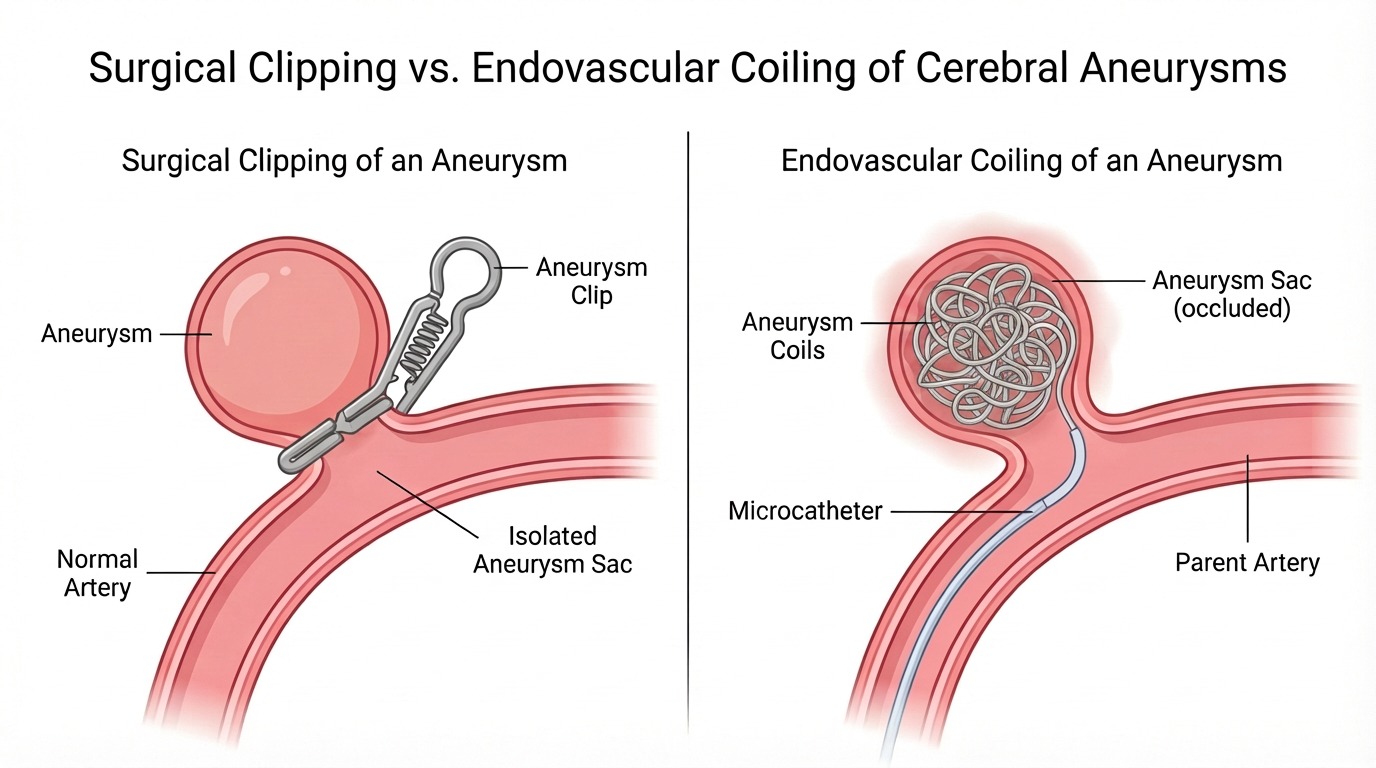
- Saccular — the common “berry” type. A round or lobed pouch off a parent vessel. Most are treated by coiling, stent-assisted coiling, or a flow diverter; some by clipping.
- Fusiform — the artery itself is dilated over a length, with no clear neck. Often treated with a flow diverter or vessel reconstruction.
- Dissecting — a tear in the artery wall lets blood track between layers. Management is different again, often involving stent or flow diverter and antiplatelet therapy in the unruptured case. Ruptured dissecting aneurysms (especially of the vertebral artery) are a neurovascular emergency managed urgently in hospital.
Most aneurysms are small (under 10 mm) and many never produce symptoms. The clinically important questions for any aneurysm are: how big, where, what shape, and what’s your individual risk.
Symptoms and warning signs
Is a brain aneurysm a medical emergency?
An unruptured aneurysm is usually not an emergency — many are found incidentally and managed as outpatients with surveillance or planned treatment. A ruptured aneurysm is a life-threatening emergency. A sudden, “worst-ever” thunderclap headache — especially with neck stiffness, vomiting, sudden weakness, or loss of consciousness — needs immediate 000 response.
Most unruptured aneurysms cause no symptoms at all and are found incidentally on a scan ordered for an unrelated reason — migraines, head injury, sinus disease.
Larger aneurysms can press on nearby structures and produce:
- Pain above or behind one eye
- Double vision or a drooping eyelid (third-nerve palsy)
- Numbness or weakness on one side of the face
- A persistent headache that is new for you
A ruptured aneurysm is a different story. The classic presentation is the “thunderclap headache” — a sudden explosive headache that hits peak intensity within seconds and is unlike anything the person has felt before. It is often accompanied by neck stiffness, vomiting, sensitivity to light, confusion, sudden weakness, seizures, or loss of consciousness.
Causes and risk factors
Brain aneurysms develop from an interaction of vessel-wall biology and lifelong haemodynamic stress. Some factors you can change; some you can’t.
You can’t change:
- Family history — a first-degree relative with an intracranial aneurysm increases your risk severalfold.
- Genetic conditions — autosomal dominant polycystic kidney disease, Ehlers-Danlos type IV, and connective tissue disorders such as Marfan syndrome.
- Sex — women have a moderately higher prevalence of unruptured intracranial aneurysms than men.
- Age — most are diagnosed between 35 and 60.
- Infective endocarditis — a small fraction of aneurysms are mycotic (infectious). These are managed jointly with infectious diseases and often need treatment of both the infection and the aneurysm.
You can change:
- Blood pressure — the most important modifiable factor for both formation and rupture.
- Smoking — roughly doubles rupture risk and accelerates aneurysm growth. Quitting reverses some of that risk over time.
- Heavy alcohol — sustained heavy drinking weakens vessel walls and raises blood pressure.
- Cocaine and methamphetamine — cause dangerous transient pressure spikes; absolute avoidance.
How it’s diagnosed
Three imaging modalities matter, and they’re used in different situations:
CT angiography (CTA)CT angiography (CTA)A rapid, non-invasive scan using iodinated contrast to image blood vessels. First-line in suspected ruptured aneurysm or acute symptoms. — rapid, widely available, first-line in any suspected acute rupture or new neurological symptoms. Sensitivity for aneurysms 3 mm or larger is excellent.
MR angiography (MRA)MR angiography (MRA)Magnetic resonance angiography. Uses MRI (no radiation, no iodinated contrast in the time-of-flight technique) to image cerebral blood vessels. Surveillance modality of choice for known unruptured aneurysms. — the surveillance modality of choice for known unruptured aneurysms. No radiation. Time-of-flight MRA needs no intravenous contrast in many patients.
Digital subtraction angiography (DSA)Digital subtraction angiography (DSA)The gold-standard catheter-based angiogram. A thin catheter is passed from a wrist or groin puncture to the cerebral arteries; contrast is injected and X-ray imaging captures the vessels in fine detail. Used for treatment planning and during endovascular treatment itself. — the gold-standard catheter angiogram. We use it for treatment planning and during the endovascular procedure itself. It is no longer routine for surveillance of small stable aneurysms.
How rupture risk is judged. A flat “under 1 percent per year” rule is too crude. We use the PHASES score (and, for treatment-vs-watch decisions, the UIATSUIATSUnruptured Intracranial Aneurysm Treatment Score — a structured framework that integrates patient, aneurysm, and treatment-related factors to support the decision to treat or observe. framework) to estimate individual rupture risk. PHASES gives a 5-year cumulative rupture risk from six factors: Population, Hypertension, Age, aneurysm Size, Earlier subarachnoid haemorrhage, and Site (location). UIATS additionally weights smoking, family history, lobulation and other factors when the treat-vs-watch call is borderline. Posterior-circulation and posterior-communicating aneurysms under 7 mm carry materially higher risk than anterior-circulation aneurysms of equivalent size (PHASES groups posterior-communicating aneurysms with the posterior circulation for scoring).
Treatment — what we do, and what we refer
Three pathways: surveillance, endovascular treatment, and microsurgical clipping. The right choice depends on the aneurysm and the patient.
Surveillance — when watching is the right answer
For many small (typically <7 mm), stable, anterior-circulation aneurysms in patients without high-risk features, the safest option is active surveillance: scheduled MRA at agreed intervals, blood-pressure optimisation, smoking cessation support, and a re-evaluation if anything about the aneurysm or you changes.
Endovascular treatment — performed by CURA’s team
Performed through a small puncture in the radial artery (wrist) or femoral artery (groin), under general anaesthesia. No skull opening. Hospital stay is typically 1–2 nights.
- Coiling — soft platinum coils are packed into the aneurysm sac, prompting clotting and sealing it from circulation.
- Stent-assisted coiling and balloon-assisted coiling — for wide-necked aneurysms where bare coiling won’t hold.
- Flow diverters — finely woven stent-like meshes that redirect blood flow away from the aneurysm, triggering it to thrombose and the parent vessel to remodel. Particularly useful for large or giant ICA-segment aneurysms.
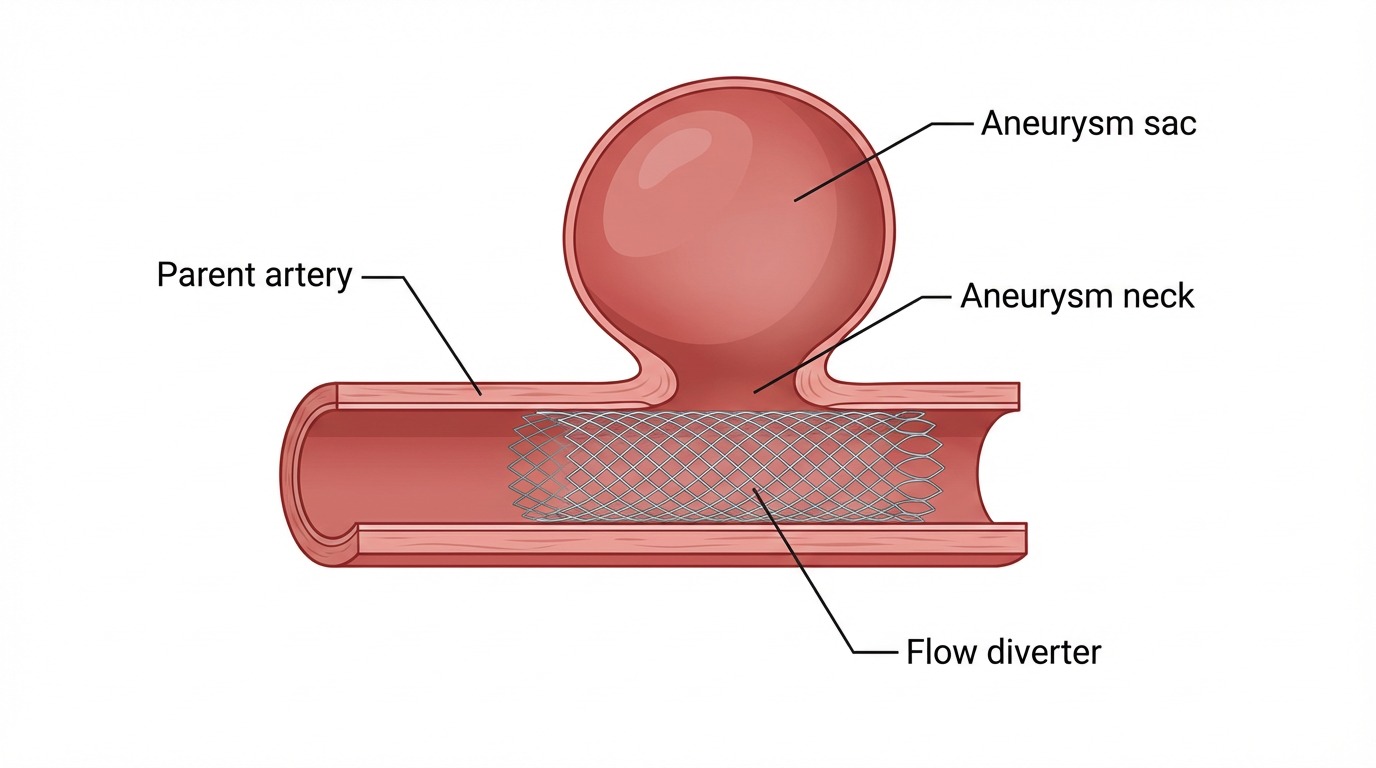
A flow diverter is a fine braided mesh stent placed inside the parent artery across the aneurysm neck — redirecting blood flow and prompting the aneurysm to thrombose. - Woven EndoBridge (WEB)Woven EndoBridge (WEB)An intrasaccular device deployed inside the aneurysm sac itself. Particularly useful for wide-necked bifurcation aneurysms (MCA bifurcation, AComm, basilar tip) where coils and stents are less ideal. and other intrasaccular devices — for wide-necked bifurcation aneurysms (MCA bifurcation, AComm, basilar tip).
Microsurgical clipping — referred to neurosurgical colleagues
CURA’s interventional neurology and neuroradiology team do not perform open craniotomy. Where clipping is the better option — some MCA bifurcation aneurysms with unfavourable necks, very small lesions unsuitable for endovascular devices, or specific complex configurations — we refer to and co-manage with established Sydney neurosurgical units. The neurosurgeon performs the clipping; CURA remains your home base for follow-up imaging and surveillance.
Living with an unruptured aneurysm
The most powerful thing you can do is control your blood pressure. Closely followed by stopping smoking. Together, these two changes do more to reduce your rupture risk than almost anything else.
What is generally fine for most patients with a small, stable, unruptured aneurysm:
- Regular aerobic exercise (lowers blood pressure long-term)
- Working, including manual work in most cases
- Sex
- Air travel
- Moderate weight training
What to avoid:
- Cocaine and methamphetamine — absolute avoidance, dangerous pressure spikes
- Heavy binge drinking — spikes blood pressure and weakens vessel walls
- Smoking — if you do nothing else, stop this
For larger, complex, or recently treated aneurysms, restrictions are individualised — ask at your consultation.
Pregnancy. A small, stable, unruptured aneurysm is generally not a contraindication to pregnancy or to vaginal delivery. Mode of delivery is decided jointly with obstetrics. Newly diagnosed or symptomatic aneurysm in pregnancy is managed case-by-case.
Should my family be screened?
MRA screening is generally recommended when:
- You have two or more first-degree relatives (parent, sibling, or child) with a confirmed intracranial aneurysm or aneurysmal subarachnoid haemorrhage.
- You have autosomal dominant polycystic kidney disease — screening is offered through joint renal/neurology pathways.
A single affected first-degree relative is also considered for screening — particularly when the affected relative is under about 60, when their event was an aneurysmal subarachnoid haemorrhage rather than an incidental finding, or when the patient has a personal history of SAH. The decision weighs family history detail, patient preference, and the lower yield in this group.
Initial screening is typically in the 20s or 30s. If the first scan is clear, repeat imaging is offered at intervals tailored to your family history and individual risk, generally ceasing in older age unless treatment would still be considered.
After treatment
After endovascular coiling. Follow-up MRA or DSA is individualised. A typical schedule is around 6 months, then 1, 3 and 5 years to confirm continued aneurysm occlusion. Earlier or extra imaging is added when occlusion is incomplete or the case is complex.
After flow-diverter placement. Imaging at 3–6 months and 12 months is typical, to confirm aneurysm occlusion and parent-vessel patency, then less frequent risk-adapted surveillance.
Antiplatelet therapy. Stent-assisted coiling and flow-diverter procedures require dual antiplatelet therapy — aspirin plus clopidogrel (or ticagrelor) — commenced before the procedure and continued for several months afterwards (typical durations range from 3 to 12 months depending on the device and individual case), with a long-term aspirin tail. Pre-procedure platelet-function testing (e.g. VerifyNow / P2Y12) is used to confirm clopidogrel responsiveness, with a switch to ticagrelor or prasugrel if hyporesponsive. Your specific regimen is set at consultation.
At your consultation
A first neurovascular consultation usually takes 45–60 minutes.
Bring
- Your GP referral letter
- Your imaging on USB or CD, plus the radiology report
- A current medication list (including over-the-counter and supplements)
- Recent blood pressure readings if you have them
- Medicare card and any private health insurance details
- A family member or friend — a second pair of ears is invaluable
What we’ll do
- Review your scans together with you
- Calculate your individualised rupture risk (PHASES, with UIATS for borderline cases)
- Discuss surveillance vs treatment options in plain language
- Agree the next imaging cadence
- Provide a written letter to your GP
Fees and wait time
Consultation fees and out-of-pocket gaps depend on consultation type and your Medicare and private-health eligibility. Wait times depend on triage urgency — symptomatic or high-risk presentations are triaged urgently. For current fees and availability, please call our reception or use the online booking page.
Frequently asked questions
I have just been told I have a brain aneurysm — am I going to die?
Almost certainly not from this. Most brain aneurysms never rupture — particularly the small ones found incidentally. Five-year rupture risk under PHASES is often well under 5% for small anterior-circulation aneurysms. Your individual risk is calculated from your aneurysm’s location and size, your age, blood pressure, prior subarachnoid haemorrhage, and population factors (the PHASES score), with extra weighting for smoking and family history under UIATS. Take the time to get a specialist consultation and a clear plan — that’s the right next step.
Will my aneurysm rupture?
Probably not, but the honest answer is: it depends on the aneurysm and on you. We use the PHASES score to estimate 5-year rupture risk from six factors. Size matters, but so does location — posterior-communicating and posterior-circulation aneurysms under 7 mm carry higher risk than anterior-circulation aneurysms of the same size. We’ll walk through your specific numbers at the consultation.
Does CURA do the procedure or refer me to a neurosurgeon?
For endovascular treatments — coiling, stent-assisted coiling, flow diverters, intrasaccular devices — Dr Winters, Dr Ang, Dr Bhatia and Dr Harrison personally perform the procedures at affiliated Sydney hospitals. Open microsurgical clipping is performed by neurosurgical colleagues; we co-manage these patients and remain your home base for follow-up imaging and surveillance.
Can I fly, drive, lift weights, or have sex with an unruptured aneurysm?
For most patients with a small, stable, unruptured aneurysm, regular life is encouraged — including aerobic exercise, work, sex, and air travel. Controlling blood pressure is the single most important thing you can do. Cocaine and methamphetamine cause dangerous transient pressure spikes and should be avoided absolutely. Specific restrictions are individualised at your consultation.
Do I need a GP referral to see you?
Yes — a current GP referral is required to claim the Medicare rebate on your specialist consultation. A referral from your GP is valid for 12 months; from another specialist, 3 months.
How quickly can I be seen?
Symptomatic and high-risk presentations are triaged urgently. Routine new-referral wait times depend on current clinic load — please call our reception for live availability at our Drummoyne and Penrith locations, or book online and our team will confirm the next available slot.
What does the consultation cost?
Fees depend on consultation type and your Medicare and private-health eligibility. Our reception team will confirm the consultation fee, expected Medicare rebate, and typical out-of-pocket gap when you book.
Should my family members be screened?
Yes if you have two or more first-degree relatives with a confirmed intracranial aneurysm or aneurysmal subarachnoid haemorrhage, or if you have autosomal dominant polycystic kidney disease. Case-by-case with a single affected first-degree relative. MRA is the screening test of choice.
Coiling vs clipping — which is right for me?
Both are effective. Endovascular coiling (and modern alternatives like flow diverters or the Woven EndoBridge) is minimally invasive and suits most aneurysms today. Microsurgical clipping is preferred for some MCA bifurcation aneurysms with unfavourable necks, very small lesions unsuitable for devices, or specific complex configurations. The decision is made by multidisciplinary discussion of your specific aneurysm.
What happens after my aneurysm is treated?
Follow-up imaging at scheduled points (typically 6 months, 1, 3 and 5 years after coiling; 3–6 and 12 months after a flow diverter) to confirm continued occlusion. Stent and flow-diverter cases involve dual antiplatelet therapy for several months, then aspirin alone long-term. Your specific cadence is set at consultation.
For referring GPs
Who is appropriate for CURA outpatient
- Incidentally found unruptured intracranial aneurysm
- Known aneurysm requiring second opinion or surveillance
- Family screening (two first-degree relatives, or ADPKD)
- Post-treatment surveillance (transferred care or shared care)
When to send to ED instead
- Sentinel or thunderclap headache — CT/CTA and neurosurgical input the same day
- Acute focal neurological deficit — suspected stroke / SAH pathway
- Reduced level of consciousness — 000
How to refer
Referrals are accepted via secure messaging, fax, and email. For current HealthLink EDI, fax and email details, please contact our reception or visit the Refer a Patient page.
What to include in the letter
- History, modifiable risk factors, family history of SAH or aneurysm, ADPKD status
- Recent BP readings, smoking status
- Imaging report — CTA preferred, MRA acceptable; please include the source images on disc or via secure link if recent imaging is available
- Current medication list (especially anticoagulants and antiplatelets)
What we send back
A written consultation letter to the referring GP, with imaging recommendations, individualised PHASES-based risk assessment, surveillance plan, and a clear plan for shared care.
Triage and wait times
Symptomatic and high-risk presentations are triaged urgently. Routine new-referral wait times depend on current clinic load — please call our reception for live availability or to flag urgency on a specific referral.
Your Sydney neurovascular team




Patient resources
- Brain Foundation Australia — brainfoundation.org.au
- Stroke Foundation Australia — strokefoundation.org.au (StrokeLine 1800 787 653)
- Healthdirect Australia — healthdirect.gov.au — brain aneurysm
- NSW Ambulance — 000 for any emergency
CURA Medical Specialists — neurovascular care in Drummoyne, Sydney’s Inner West. Book a consultation · For referring GPs