Carpal Tunnel Syndrome
Diagnosis and treatment in Sydney — a guide for patients and referring GPs

Tap or hover any dotted-underlined term for a plain-English definition.
Most people with carpal tunnel get better without surgery. What you need first is a clear diagnosis — and that means a nerve test that grades how compressed the nerve actually is.
- Tingling or numbness in your thumb, index or middle finger — rarely the little finger
- Symptoms that wake you at night, or come on while driving or holding a phone
- Shaking your hand makes it feel better
- Dropping objects, weak grip, or trouble doing up buttons
- Symptoms in one hand more than the other — often the dominant side first
- If two or more apply, an in-clinic nerve conduction study can confirm it and grade severity — which decides the right treatment.
Your visit at CURA — what to expect
Before the visit
- Ask your GP for a referral so Medicare rebates apply (a GP referral is valid for 12 months; from another specialist, 3 months).
- Make a short note of when symptoms started, which hand, and what makes them worse (typing, driving, sleeping).
Consultation and nerve conduction study — usually two separate bookings
A consultation and a nerve conduction study (NCS) are usually booked as two separate appointments. Some patients are fortunate enough to have both done on the same day, but this is not the norm.
What you want is decided when your GP writes the referral. Please make it clear from the outset whether you want a consultation, a nerve study, or both — otherwise you may need to come back for one or the other.
If you book a nerve conduction study only, the feedback at the end of the test is brief. Time constraints mean we cannot deliver a full consultation within an NCS session. If you want both the test and a full discussion of treatment, please request both at the time of referral.
What you leave with
- From a consultation: a treatment plan, a written report to your GP, and any onward referrals that are needed.
- From a nerve study: a brief summary of the result and a written report to the referring GP. Detailed discussion of what the result means and what to do next happens at a consultation.
If surgery is the right call
- CURA does not perform carpal tunnel release. We coordinate referral to an experienced hand surgeon and supply your full NCS report so they have everything they need.
- Both open and endoscopic (keyhole) release are widely performed in Australia — long-term outcomes are similar; endoscopic typically means a faster early return to work.
Most people with mild or moderate CTS never reach the surgical step.
What carpal tunnel syndrome is
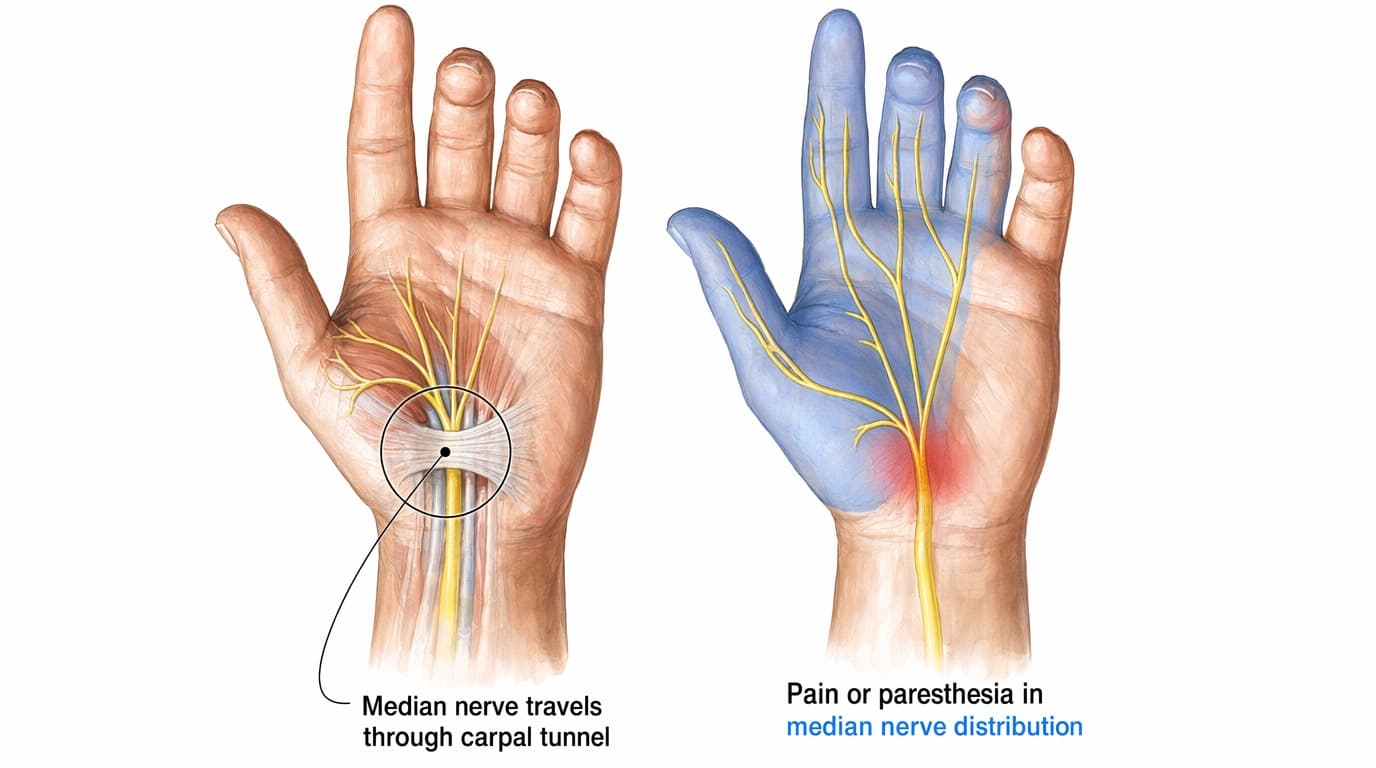
Carpal tunnel syndrome happens when one of the nerves to your hand gets squeezed at the wrist.
That nerve is the median nervemedian nerveOne of three main nerves in the arm. It supplies feeling to your thumb, index, middle and half of the ring finger, and powers a few of the muscles at the base of your thumb.. The carpal tunnelcarpal tunnelA narrow channel of bone and ligament at the front of your wrist. The median nerve and the tendons that bend your fingers all pass through it. is the narrow passageway at the front of your wrist that the nerve passes through. When pressure builds inside the tunnel, the nerve sends garbled signals. You feel tingling, burning, or numbness. Over time, weakness can follow.
CTS is the most common entrapment neuropathy in Australian adults. It’s particularly common in:
- Adults aged 40–60, especially women
- People with diabetes, thyroid disease, rheumatoid arthritis, or kidney disease
- Pregnancy (often resolves after birth, due to fluid retention)
- Occupations involving sustained or repetitive wrist movement — keyboard work, manual trades, hairdressing, music performance
- Following wrist fractures or sustained vibration exposure
Symptoms and red flags
Typical pattern
- Pins and needles or numbness in the thumb, index, middle and half of the ring finger
- Pain or burning in the wrist that may radiate up the forearm
- Worse at night and on waking — many patients wake repeatedly to “shake the hand back to life”
- Provoked by driving, holding a phone, reading a book, or any sustained wrist position
- Eventually, weakness or clumsiness — especially fine pinch (turning a key, doing up buttons)
Conditions that can look similar
Tingling and numbness in the hand isn’t always carpal tunnel. A neurologist’s job is to make sure we’re treating the right problem. Common look-alikes:
- A pinched nerve in your neck (cervical radiculopathycervical radiculopathyNerve irritation where it leaves your spinal cord in the neck. C6 and C7 are the levels that most often mimic carpal tunnel.) — usually at the C6 or C7 spinal level. Causes hand and forearm tingling, often with neck or shoulder pain.
- The same median nerve trapped higher up, in the forearm — pronator or anterior interosseous syndrome. Same nerve, different location.
- Nerve damage affecting both hands and feet at once (peripheral neuropathyperipheral neuropathyDiffuse nerve damage typically affecting the hands and feet symmetrically. Diabetes is the most common cause in Australia.) — most often seen with diabetes.
- A trapped nerve at the elbow (cubital tunnel syndrome) — affects your little and ring finger, not your thumb.
- A nerve injury near your collarbone — a brachial plexus problem. The brachial plexus is the bundle of nerves that leaves your spine and runs to your arm.
Treating “CTS” that’s actually cervical radiculopathy with a wrist splint won’t help — which is why a careful examination, sometimes alongside nerve conduction studies, matters.
How we diagnose carpal tunnel at CURA
1. We start by listening
We ask about the pattern, timing, and triggers of your symptoms, and review your medical conditions and medications. Where appropriate, we examine the hand — sensation, the bulk and strength of the thumb-base muscles, and bedside provocative tests (such as Tinel’s, Phalen’s or Durkan’s). The specific tests performed at any given visit are at the clinician’s discretion and depend on the presentation; not every test is elicited at every consultation.
2. The nerve test (NCS and EMG)
The nerve test is the most reliable way to confirm CTS (AANEM / AAN / AAPM&R Practice Parameter — Jablecki et al.). We do it on-site — no separate hospital trip. There are two parts:
- NCS (nerve conduction study). Small electrical pulses measure how fast and how strongly signals travel along the median nerve. We compare your symptomatic hand to typical values, and to your other hand.
- EMG (electromyography). A fine needle checks whether the muscles your median nerve controls are losing signal. If they are, the compression is more advanced.
The test does more than confirm CTS. It grades how compressed the nerve is. The grade decides the right treatment.
3. Ultrasound and MRI — not routine
We do not routinely order ultrasound or MRI for carpal tunnel syndrome. Imaging may be performed in unique circumstances — for example, suspicion of a ganglion cyst or mass, an atypical presentation, or symptoms that return after surgery. Sometimes imaging has already been organised by your GP before the referral. If we think imaging is needed, we’ll explain why.
4. Blood tests
We may check for things that make CTS worse — usually thyroid function, blood sugar (HbA1c), and inflammation markers. Treating the underlying cause can improve symptoms and reduce recurrence.
What mild, moderate, and severe mean for you
Your nerve test gives you a severity grade. We talk about your result in three plain-language groups:
- Mild — splinting and activity changes are usually enough.
- Moderate — splinting first; we may consider a steroid injection if it doesn’t help.
- Severe — straight to a surgeon. The nerve has been squeezed long enough to start losing function, so a splint trial isn’t the right next step.
For your GP and report: this three-way grouping is CURA’s reporting convention. Underneath it we use the six-grade Bland scaleBland scaleA six-grade neurophysiology severity scale for carpal tunnel syndrome — from 1 (very mild, sensory slowing only) to 6 (no recordable signal). Bland, Muscle & Nerve, 2000. — a standard neurophysiology tool (Muscle & Nerve, 2000). Grades 1–2 map to mild, 3–4 to moderate, 5–6 to severe. The Bland grade itself appears in your written report.
Treatment — most people don’t need surgery
The right treatment depends on your nerve-test severity grade, how long you’ve had symptoms, and what’s driving them.
The exception: if the nerve test is severe, or there’s already muscle wasting at the base of the thumb, splinting won’t fix it. You go straight to a surgeon.
Conservative care — first line for mild and most moderate cases
- Night-time wrist splints in a neutral position — the simplest and best-evidenced first step. Pregnancy CTS usually responds well. A neutral-position night splint is inexpensive; the easiest way to find one is to search “CTS splint” on Amazon (or any similar retailer) — you don’t need anything specialised to start.
- Activity modification and ergonomics — neutral wrist posture at the keyboard, regular breaks, avoiding sustained gripping. (High-quality evidence specifically for ergonomic interventions is modest, but they remain a sensible adjunct.)
- Treating underlying conditions — diabetes, hypothyroidism, inflammatory arthritis.
- Hand therapy — tendon-gliding and nerve-gliding exercises, plus splint fitting.
A trial of night splinting (typically 4–6 weeks) is a reasonable first step in mild or moderate CTS. (This timeframe is practice convention rather than a fixed rule.) If symptoms aren’t improving — or if any red flag appears — we move on.
Steroid injection — selected moderate cases
A steroid injection into the carpal tunnel can give real short-term relief (Marshall Cochrane review; Atroshi 2013, JAMA). It can also delay or avoid surgery in selected patients.
It’s not a cure. Symptoms come back within a year for many people. It’s most useful when you want to defer surgery (for example, in late pregnancy), or when the CTS is moderate and looks more inflammatory than mechanical. CURA coordinates referral to a proceduralist for an ultrasound-guided injection where indicated.
Surgery — carpal tunnel release
Surgery is the right next step in three situations:
- The nerve test is severe-grade
- There’s muscle wasting at the base of your thumb, or fixed numbness
- Splinting hasn’t helped after a fair trial in mild or moderate CTS
This is supported by the AAOS Clinical Practice Guideline.
We don’t do the surgery ourselves. CURA is a neurology and nerve-testing practice. When surgery is indicated, we coordinate referral to an experienced hand surgeon and send your full nerve-test report.
There are two types of release surgery: open and endoscopic (keyhole). Both are widely done in Australia. Long-term results are similar. Endoscopic release usually means a faster early return to work. Your hand surgeon will discuss which approach suits you.
Carpal tunnel in pregnancy
Pregnancy-related CTS is common — fluid retention raises pressure inside the carpal tunnel. The good news: most cases settle after birth.
- Night-time splinting is first-line and is safe in pregnancy.
- Steroid injection or surgery are usually deferrable until after birth.
- If symptoms are severe, we’ll discuss the safest plan with you and your obstetric team.
Frequently asked questions
Can carpal tunnel syndrome resolve without surgery?
Yes. Most mild-to-moderate cases at CURA improve with night splinting, activity changes, and treating any underlying condition (diabetes, thyroid disease, inflammation).
Surgery is considered when:
- The nerve test is severe-grade
- Conservative care hasn’t worked in milder cases
- There’s muscle wasting or fixed numbness — we refer directly, no splint trial first
How is carpal tunnel syndrome diagnosed?
A neurologist takes a detailed history, and where appropriate examines your hand and wrist using bedside provocative tests. The diagnosis is confirmed with the nerve conduction study (NCS) and EMG.
At CURA, the nerve test is done on-site by our Clinical Neurophysiologists — Dr El-Wahsh, FRACP, Dr Vo, FRACP, and Dr Swart, FRACP.
Is the consultation and the nerve study one appointment or two?
Usually two. A consultation and a nerve conduction study are typically booked as separate appointments. Some patients do have both done on the same day, but this is not the norm. Decide what you want at the time of referral — consultation, nerve study, or both — otherwise you may need to come back for one or the other.
If you book a nerve study only, the feedback at the end of the test is brief. We can’t deliver a full consultation within an NCS session due to time constraints.
Does Medicare cover carpal tunnel assessment at CURA?
Yes. Specialist neurology consultations attract Medicare rebates for both face-to-face and telehealth visits. Nerve conduction studies and EMG attract a rebate under the relevant MBS item (commonly 11018). See our fees page for current gap fees, or call reception.
How long does the nerve conduction test take, and does it hurt?
The NCS / EMG study takes about 30–45 minutes. Most people describe the small electrical pulses as a brief “tap” or tingle — uncomfortable but not painful. The needle component of EMG, when needed, is well tolerated and usually short. Feedback at the end of the test is brief; detailed discussion of the result happens at a consultation.
Will I need surgery?
Most people don’t. Surgery is recommended when:
- The nerve test is severe-grade
- The muscles your nerve controls are losing signal
- Splinting hasn’t worked
- There’s already visible muscle wasting at the base of your thumb
Even in moderate cases, many people improve with splinting and activity change alone.
How long does recovery from carpal tunnel surgery take?
Most people are using the hand for light tasks within days. Typical timelines:
- Return to office work — around 2 weeks
- Return to manual work — 6–8 weeks (depending on the type of release and how heavy the work is)
- Full nerve recovery — months, especially if CTS was long-standing or severe
Your hand surgeon will give you timelines that fit your job and surgery type.
Can carpal tunnel syndrome be prevented?
Not always, but you can lower your risk:
- Keep your wrist in a neutral (straight) position when you can
- Take regular breaks from sustained gripping or typing
- Treat underlying conditions like diabetes and thyroid problems
- Address CTS early in pregnancy
Some risk is genetic or anatomical and can’t be prevented.
Do I need a GP referral?
A GP referral is required to claim a Medicare rebate on your specialist consultation. We’re happy to see private patients without a referral, but the rebate won’t apply. A GP referral is valid for 12 months; from another specialist, 3 months.
For referring GPs
Clinical lead
- Dr Shadi El-Wahsh, FRACP, Clinical Neurophysiologist
- Also seeing CTS: Dr Henry Vo, FRACP, Dr Grace Swart, FRACP (both Clinical Neurophysiologists)
How to refer
Address: “CURA Medical Specialists — Neurology, attn. Clinical Neurophysiology team (CTS / NCS).” A named-doctor referral is not required — we triage to the next available neurophysiologist.
Referrals accepted via secure messaging, fax, and email. For current HealthLink EDI, fax and email details, please contact reception or visit the Refer a Patient page.
Please include in the letter
- Symptom duration and laterality, night symptoms
- Tinel / Phalen / Durkan result, presence/absence of thenar wasting
- Comorbidities — diabetes, thyroid disease, pregnancy, RA
- Prior splinting, injection trials, occupation
What we do at CURA
- Specialist consultation plus on-site NCS / EMG where slotting allows
- Written report back to the GP within standard turnaround
- If surgery is indicated: we coordinate onward referral to an experienced hand surgeon and supply the NCS report
MBS
Specialist neurology consultations attract Medicare rebates under the standard initial / review items (face-to-face and telehealth equivalents). NCS / EMG attract a rebate under the relevant MBS item (commonly 11018). See our fees page for current consultation and study fees, or call reception.
Locations
Drummoyne · Nepean (Penrith).
Triage and wait times
Routine NCS appointments are typically scheduled within a few weeks. Urgent presentations — thenar wasting, fixed numbness, post-trauma — are triaged urgently. Please phone reception to flag urgency on a specific referral.
Your Sydney carpal tunnel team



Patient resources
- Australian Hand Therapy Association — ahta.com.au (find an accredited hand therapist)
- Better Health Channel — Carpal tunnel syndrome (Victorian Government) — betterhealth.vic.gov.au
- HealthDirect Australia — Carpal tunnel syndrome — healthdirect.gov.au
- RACGP / AJGP — Carpal tunnel syndrome — racgp.org.au (peer-reviewed Australian primary-care reference)
- Versus Arthritis — Carpal tunnel syndrome — versusarthritis.org
- MBS Online — Services Australia — mbsonline.gov.au (current item descriptors and rebates)
CURA Medical Specialists — clinical neurophysiology and carpal tunnel care in Drummoyne & Nepean (Penrith). Book a consultation · For referring GPs